












51% of No Tau / Low Tau Patients Showed Improved Cognition and Function Over Three Years; Only Lecanemab Has Clinical Data in No Tau / Low Tau Patient Group
Clinical Data and Biomarkers Show Alzheimer’s Disease Does Not Stop Progressing After Plaque Clearance. Lecanemab’s Dual Action Supports Neuronal Function by Clearing Highly Toxic Protofibrils that Continue to Cause Neuronal Injury and Death After Rapid Plaque Clearance
Lecanemab Slows Tau Spread Across All Brain Regions
PHILADELPHIA, July 30, 2024 (GLOBE NEWSWIRE) -- Eisai Co., Ltd. (Headquarters: Tokyo, CEO: Haruo Naito, “Eisai”) and Biogen Inc. (Nasdaq: BIIB, Headquarters: Cambridge, Massachusetts, United States, CEO: Christopher A. Viehbacher, “Biogen”) announced today that the latest findings for lecanemab-irmb (U.S. brand name: LEQEMBI®), an anti-amyloid beta (Aβ) protofibril* antibody for the treatment of early Alzheimer’s disease (AD), were presented at the Alzheimer’s Association International Conference (AAIC) 2024, held in Philadelphia, USA, and virtually. Dual-acting lecanemab is the only early AD treatment widely available to support neuronal function by clearing the highly toxic protofibrils that continue to cause neuronal injury and death even after plaques have been cleared from the brain. The presentation slides for the two scientific sessions on lecanemab at the AAIC will be available on the Eisai Co. Ltd. Investor Page by 7:00 p.m. on July 30th EDT.
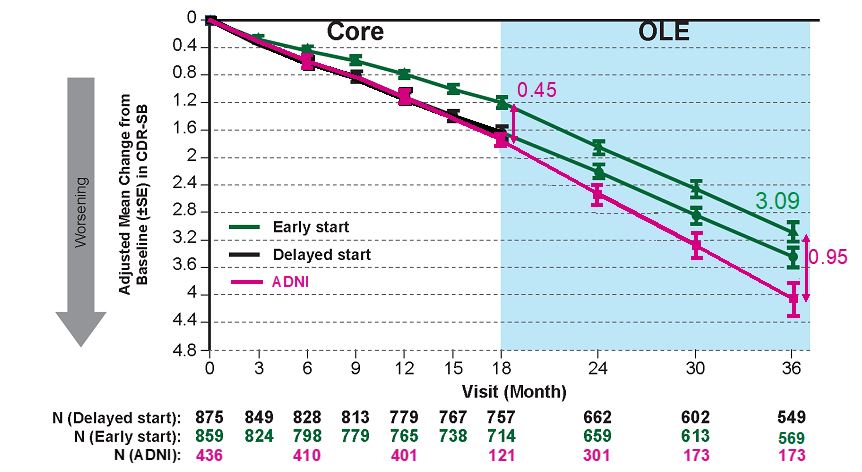
Three Years of Continuous Lecanemab Treatment Reduced Clinical Decline by -0.95 on CDR-SB Showing Continued Clinically and Personally Meaningful Benefit for Early AD Patients
Clarity AD was a global Phase 3 placebo-controlled, double-blind, parallel-group, randomized study in 1,795 people with early AD (Lecanemab group: 10 mg/kg bi-weekly IV treatment: 898, placebo group: 897). 95% of patients who completed the core study (18 months) chose to continue in the open-label extension study (OLE). In the Clarity AD core study, the mean change from baseline between the lecanemab treated group and the placebo group was -0.45 (P=0.00005) on the primary endpoint of the Clinical Dementia Rating-Sum of Boxes (CDR-SB) global cognitive and functional scale. Over three years of treatment across the core study and OLE, lecanemab reduced cognitive decline on the CDR-SB by -0.95 compared to the expected decline based on the Alzheimer’s Disease Neuroimaging Initiative (ADNI)** group.1 A change from 0.5 to 1 on the CDR score domains of Memory, Community Affairs and Home/Hobbies is the difference between slight impairment and loss of independence, such as people’s ability to be left alone, remember recent events, participate in daily activities, complete household chores, function independently and engage in hobbies and intellectual interests.2,3
Safety Matters
No new safety findings have been observed with continued lecanemab treatment over three (3) years. Most Amyloid-related imaging abnormalities (ARIA) occurred in the first six months of treatment. After the first six months, ARIA rates are low and similar to ARIA rates on placebo. Most patients who had ARIA had CDR-SB assessments after the event. Sensitivity analyses showed ARIA had no impact on cognition or function. From these results ARIA was not associated with accelerated long-term progression.1 As stated in the FDA product label, the incidence and timing of ARIA vary among treatments.4
More than 50% of Patients Who Started Treatment in the Earliest Stage of AD Continued to Show Improvement After Three Years of Lecanemab Treatment
The Clarity AD study included an optional tau PET substudy and used the tau PET probe MK6240 to identify patients with no tau or a low accumulation of tau in the brain. As tau begins to accumulate in the brain, cognition and function start to decline; therefore, patients with no tau or low tau in the brain represent an early stage of AD. After three years of lecanemab treatment, 59% of these patients (24/41) showed improvement or no decline, and 51% (21/41) showed improvement from baseline on the CDR-SB. On the ADAS-Cog14 measurement scale, 63% of patients showed improvement or no decline and 61% showed improvement. On the ADCS MCI-ADL, 63% of patients showed improvement or no decline and 59% showed improvement. This suggests that earlier initiation of treatment with lecanemab may have a significant positive impact on disease progression and may provide continued benefits to patients with early AD over the long-term.1
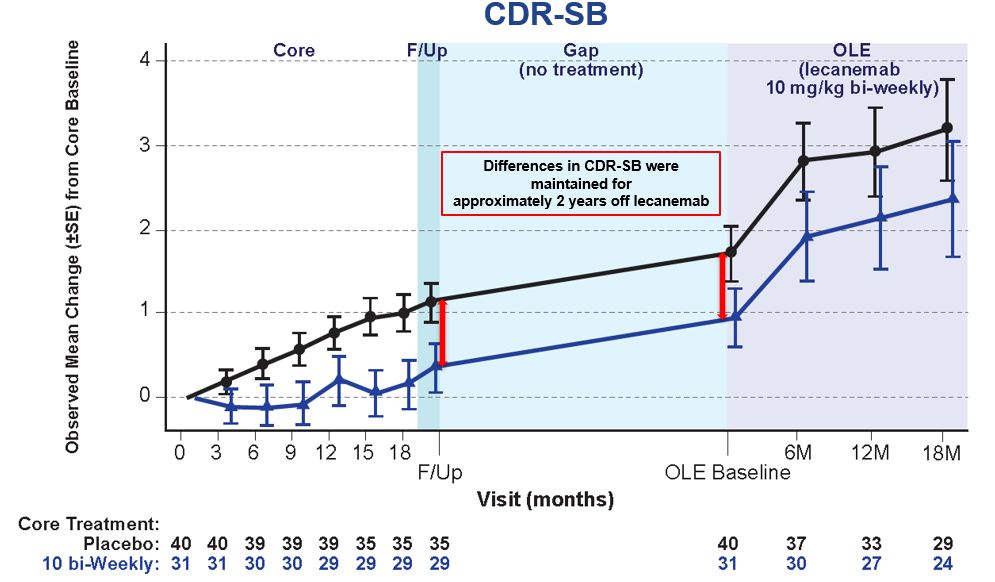
Even After Plaque Clearance, AD Continues to Progress When Treatment is Stopped
Study 201 is a multicenter, double-blind, placebo-controlled, Phase 2b trial conducted in 856 patients with early AD. Appropriate patients participated in the OLE after an off-treatment period of 9-59 months (mean: 24 months) following the 18-month core study. During the off-treatment period lecanemab’s clinical effect was maintained but the rate of decline (slope) in patients who stopped therapy reverted back to the rate of decline in patients on placebo as measured by CDR-SB. This indicates that even after Aβ plaque is removed, AD continues to progress, and reverts to the placebo rate of decline when treatment is stopped.1
After Plaque Removal, Dual-Acting Lecanemab Continues to Positively Impact Biomarkers Over the Course of Treatment
The key AD fluid biomarkers Aβ42/40, pTau181, pTau217, and glial fibrillary acidic protein (***GFAP) are more sensitive indicators of amyloid and tau development than Amyloid PET and have been shown to re-accumulate at a faster rate when treatment is discontinued. Modeling data from the Study 201 (Phase 2), Clarity AD (Phase 3) and respective OLE studies showed that the half-life of the treatment effect on the fluid biomarkers plasma Aβ42/40 ratio, pTau181, and GFAP are lost within 0.5 year, 1.6 years and 1.7 years, respectively, while the half-life of the treatment effect on amyloid plaque is gradually lost in 12.1 years. When lecanemab treatment was resumed in the Study 201 Study OLE after off-treatment period, fluid biomarkers Aβ42/40 ratio, pTau181, pTau217 and GFAP improved. These results suggest that AD continues to progress when treatment is stopped, even after plaque has been cleared. Patients continue to benefit by remaining on treatment as lecanemab maintains improvement in the fluid biomarkers of amyloid pathophysiology.1
Lecanemab’s Dual Action on Protofibrils and Plaques Impacts Amyloid and Slows Tau Spread, Offering Patients a Continuous, Long-Term Treatment for this Chronic and Progressive Disease
Lecanemab is the only widely available early AD treatment that offers a dual mechanism of action designed to selectively target highly toxic protofibrils in addition to amyloid plaques. Protofibrils accumulate early in the AD brain and lead to nerve cell function loss, abnormal nerve processes, inflammation, and memory loss. In non-clinical studies, antibodies against protofibrils prevented protofibril-mediated neuronal dysfunction and memory loss.5 Lecanemab preferentially binds to toxic protofibrils with the highest affinity. After rapidly clearing plaque and existing protofibrils, lecanemab continuously clears the protofibrils that continue to develop and damage neurons.1 Protofibrils also play a role in tau spread.5 In the tau PET substudy, continuous lecanemab treatment slowed the rate of increase in tau accumulation across all brain regions as measured by tau PET.6 CSF MTBR-tau243 has high correlation with tau PET and increases with the progression of AD pathology. Treatment with lecanemab slows the increase in CSF MTBR-tau243. Additionally, lecanemab improved pTau217 and other biomarkers related to neuroinflammation and neurodegeneration. This indicates a potential disease-modifying effect on tau pathophysiology.7
Eisai serves as the lead for lecanemab’s development and regulatory submissions globally with both companies co-commercializing and co-promoting the product and Eisai having final decision-making authority.
*Protofibrils are thought to be the most toxic Aβ species that contribute to brain damage in AD and play a major role in the cognitive decline of this progressive and devastating disease. Protofibrils can cause neuronal damage in the brain, which can subsequently adversely affect cognitive function through multiple mechanisms.5 The mechanism by which this occurs has been reported not only by increasing the formation of insoluble Aβ plaques, but also by directly damaging signaling between neurons and other cells. It is believed that reducing protofibrils may reduce neuronal damage and cognitive impairment, potentially preventing the progression of AD.8
**ADNI is a clinical research project launched in 2005 to develop methods to predict the onset of AD and to confirm the effectiveness of treatments. The ADNI observational cohort represents the exact population of those in Clarity AD study; matched ADNI participants show similar degree of decline to placebo group out to 18 months.
***Glial fibrillary acidic protein (GFAP), a marker of astroglia activation, has been proposed as a biomarker of Alzheimer’s disease (AD). GFAP expression correlates with Aβ plaque density and cerebrospinal fluid (CSF) concentration is elevated in symptomatic disease.
Please see full Prescribing Information for LEQEMBI, including Boxed WARNING.
U.S. INDICATION
LEQEMBI® [(lecanemab-irmb) 100 mg/mL injection for intravenous use] is indicated for the treatment of Alzheimer’s disease (AD). Treatment with LEQEMBI should be initiated in patients with mild cognitive impairment (MCI) or mild dementia stage of disease, the population in which treatment was initiated in clinical trials.
IMPORTANT SAFETY INFORMATION
WARNING: AMYLOID-RELATED IMAGING ABNORMALITIES (ARIA)
| |
CONTRAINDICATION
LEQEMBI is contraindicated in patients with serious hypersensitivity to lecanemab-irmb or to any of the excipients of LEQEMBI. Reactions have included angioedema and anaphylaxis.
WARNINGS AND PRECAUTIONS
AMYLOID-RELATED IMAGING ABNORMALITIES
LEQEMBI can cause ARIA-E and ARIA-H, which can occur together. ARIA-E can be observed on magnetic resonance imaging (MRI) as brain edema or sulcal effusions and ARIA-H as microhemorrhage and superficial siderosis. ARIA can occur spontaneously in patients with AD. With this class of medications, ARIA-H generally occurs in association with ARIA-E. Reported ARIA symptoms may include headache, confusion, visual changes, dizziness, nausea, and gait difficulty. Focal neurologic deficits may also occur. Symptoms usually resolve over time.
Incidence of ARIA
Symptomatic ARIA occurred in 3% (29/898) and serious ARIA symptoms in 0.7% (6/898) with LEQEMBI. Clinical ARIA symptoms resolved in 79% (23/29) of patients during the period of observation. ARIA, including asymptomatic radiographic events, was observed: LEQEMBI, 21% (191/898); placebo, 9% (84/897). ARIA-E was observed: LEQEMBI, 13% (113/898); placebo, 2% (15/897). ARIA-H was observed: LEQEMBI, 17% (152/898); placebo, 9% (80/897). No increase in isolated ARIA-H was observed for LEQEMBI vs placebo.
ApoE ε4 Carrier Status and Risk of ARIA
Of the patients taking LEQEMBI, 16% (141/898) were ApoE ε4 homozygotes, 53% (479/898) were heterozygotes, and 31% (278/898) were noncarriers. With LEQEMBI, the incidence of ARIA was higher in ApoE ε4 homozygotes (LEQEMBI: 45%; placebo: 22%) than in heterozygotes (LEQEMBI: 19%; placebo: 9%) and noncarriers (LEQEMBI: 13%; placebo: 4%). Symptomatic ARIA-E occurred in 9% of ApoE ε4 homozygotes vs 2% of heterozygotes and 1% of noncarriers. Serious ARIA events occurred in 3% of ApoE ε4 homozygotes and in ~1% of heterozygotes and noncarriers. The recommendations on management of ARIA do not differ between ApoE ε4 carriers and noncarriers.
Radiographic Findings
The majority of ARIA-E radiographic events occurred within the first 7 doses, although ARIA can occur at any time, and patients can have >1 episode. Maximum radiographic severity of ARIA-E with LEQEMBI was mild in 4% (37/898), moderate in 7% (66/898), and severe in 1% (9/898) of patients. Resolution of ARIA-E on MRI occurred in 52% of patients by 12 weeks, 81% by 17 weeks, and 100% overall after detection. Maximum radiographic severity of ARIA-H microhemorrhage with LEQEMBI was mild in 9% (79/898), moderate in 2% (19/898), and severe in 3% (28/898) of patients; superficial siderosis was mild in 4% (38/898), moderate in 1% (8/898), and severe in 0.4% (4/898) of patients. With LEQEMBI, the rate of severe radiographic ARIA-E was highest in ApoE ε4 homozygotes (5%; 7/141) vs heterozygotes (0.4%; 2/479) or noncarriers (0%; 0/278). With LEQEMBI, the rate of severe radiographic ARIA-H was highest in ApoE ε4 homozygotes (13.5%; 19/141) vs heterozygotes (2.1%; 10/479) or noncarriers (1.1%; 3/278).
Intracerebral Hemorrhage
Intracerebral hemorrhage >1 cm in diameter was reported in 0.7% (6/898) with LEQEMBI vs 0.1% (1/897) with placebo. Fatal events of intracerebral hemorrhage in patients taking LEQEMBI have been reported.
Concomitant Antithrombotic Medication:
In Clarity AD, baseline use of antithrombotic medication (aspirin, other antiplatelets, or anticoagulants) was allowed if the patient was on a stable dose. The majority of exposures to antithrombotic medications were to aspirin. Antithrombotic medications did not increase the risk of ARIA with LEQEMBI. The incidence of intracerebral hemorrhage was 0.9% (3/328) in patients taking LEQEMBI with a concomitant antithrombotic medication at the time of the event vs 0.6% (3/545) in those who did not receive an antithrombotic. Patients taking LEQEMBI with an anticoagulant alone or combined with an antiplatelet medication or aspirin had an incidence of intracerebral hemorrhage of 2.5% (2/79) vs none in patients receiving placebo. Caution should be exercised when considering the administration of anticoagulants or a thrombolytic agent (e.g., tissue plasminogen activator) to a patient already being treated with LEQEMBI.
Other Risk Factors for Intracerebral Hemorrhage:
Patients were excluded from enrollment in Clarity AD for findings on neuroimaging that indicated an increased risk for intracerebral hemorrhage. These included findings suggestive of cerebral amyloid angiopathy (prior cerebral hemorrhage >1 cm in greatest diameter, >4 microhemorrhages, superficial siderosis, vasogenic edema) or other lesions (aneurysm, vascular malformation). The presence of an ApoE ε4 allele is also associated with cerebral amyloid angiopathy. Caution should be exercised when considering the use of LEQEMBI in patients with factors that indicate an increased risk for intracerebral hemorrhage and in patients who need to be on anticoagulant therapy.
ARIA Monitoring and Dose Management Guidelines
Obtain a recent baseline brain MRI prior to initiating treatment with LEQEMBI and prior to the 5th, 7th, and 14th infusions. Enhanced clinical vigilance for ARIA is recommended during the first 14 weeks of treatment with LEQEMBI. Depending on ARIA-E and ARIA-H clinical symptoms and radiographic severity, use clinical judgment when considering whether to continue dosing or to temporarily or permanently discontinue LEQEMBI. If a patient experiences ARIA symptoms, clinical evaluation should be performed, including MRI if indicated. If ARIA is observed on MRI, careful clinical evaluation should be performed prior to continuing treatment.
HYPERSENSITIVITY REACTIONS
Hypersensitivity reactions, including angioedema, bronchospasm, and anaphylaxis, have occurred with LEQEMBI. Promptly discontinue the infusion upon the first observation of any signs or symptoms consistent with a hypersensitivity reaction and initiate appropriate therapy.
INFUSION-RELATED REACTIONS (IRRs)
IRRs were observed—LEQEMBI: 26% (237/898); placebo: 7% (66/897)—and the majority of cases with LEQEMBI (75%, 178/237) occurred with the first infusion. IRRs were mostly mild (69%) or moderate (28%) in severity. IRRs resulted in discontinuation of LEQEMBI in 1% (12/898). Symptoms of IRRs included fever and flu-like symptoms (chills, generalized aches, feeling shaky, and joint pain), nausea, vomiting, hypotension, hypertension, and oxygen desaturation.
In the event of an IRR, the infusion rate may be reduced or the infusion may be discontinued and appropriate therapy initiated as clinically indicated. Consider prophylactic treatment prior to future infusions with antihistamines, acetaminophen, nonsteroidal anti-inflammatory drugs, or corticosteroids.
ADVERSE REACTIONS
The most common adverse reaction leading to discontinuation of LEQEMBI was ARIA-H microhemorrhages that led to discontinuation in 2% (15/898) with LEQEMBI vs <1% (1/897) with placebo.
The most common adverse reactions reported in ≥5% with LEQEMBI (N=898) and ≥2% higher than placebo (N=897) were IRRs (LEQEMBI: 26%; placebo: 7%), ARIA-H (LEQEMBI: 14%; placebo: 8%), ARIA-E (LEQEMBI: 13%; placebo: 2%), headache (LEQEMBI: 11%; placebo: 8%), superficial siderosis of central nervous system (LEQEMBI: 6%; placebo: 3%), rash (LEQEMBI: 6%; placebo: 4%), and nausea/vomiting (LEQEMBI: 6%; placebo: 4%).
| MEDIA CONTACTS | |
| Eisai Co., Ltd. Public Relations Department TEL: +81 (0)3-3817-5120 Eisai Inc. (U.S.) Libby Holman + 1-201-753-1945 Libby_Holman@eisai.com Eisai Europe, Ltd. (UK, Europe, Australia, New Zealand and Russia) EMEA Communications Department +44 (0) 786 601 1272 EMEA-comms@eisai.net | Biogen Inc. Jack Cox + 1-781-464-3260 public.affairs@biogen.com |
| INVESTOR CONTACTS | |
| Eisai Co., Ltd. Investor Relations Department TEL: +81 (0) 3-3817-5122 | Biogen Inc. Chuck Triano + 1-781-464-2442 IR@biogen.com |
[Notes to editors]
1. About LEQEMBI
LEQEMBI (generic name: lecanemab) is the result of a strategic research alliance between Eisai and BioArctic. It is a humanized immunoglobulin gamma 1 (IgG1) monoclonal antibody directed against aggregated soluble (protofibril) and insoluble forms of amyloid-beta (Aβ).
LEQEMBI’s FDA approval was based on Phase 3 data from Eisai’s, global Clarity AD clinical trial, in which it met its primary endpoint and all key secondary endpoints with statistically significant results.9,10 The primary endpoint was the global cognitive and functional scale, Clinical Dementia Rating Sum of Boxes (CDR-SB). In the Clarity AD clinical trial, treatment with LEQEMBI reduced clinical decline on CDR-SB by 27% at 18 months compared to placebo. The mean CDR-SB score at baseline was approximately 3.2 in both groups. The adjusted least-squares mean change from baseline at 18 months was 1.21 with LEQEMBI and 1.66 with placebo (difference, −0.45; 95% confidence interval [CI], −0.67 to −0.23; P<0.001). In addition, the secondary endpoint from the AD Cooperative Study-Activities of Daily Living Scale for Mild Cognitive Impairment (ADCS-MCI-ADL), which measures information provided by people caring for patients with AD, noted a statistically significant benefit of 37% compared to placebo. The adjusted mean change from baseline at 18 months in the ADCS-MCI-ADL score was −3.5 in the LEQEMBI group and −5.5 in the placebo group (difference, 2.0; 95% CI, 1.2 to 2.8; P<0.001). The ADCS MCI-ADL assesses the ability of patients to function independently, including being able to dress, feed themselves and participate in community activities. The most common adverse events (>10%) in the LEQEMBI group were infusion reactions, ARIA-H (combined cerebral microhemorrhages, cerebral macrohemorrhages, and superficial siderosis), ARIA-E (edema/effusion), headache, and fall.
LEQEMBI is approved in the U.S., Japan, China, South Korea, Hong Kong and Israel for the treatment of MCI due to AD and mild AD dementia. Eisai has also submitted applications for approval of LEQEMBI in 12 countries and regions. A supplemental Biologics License Application (sBLA) for intravenous maintenance dosing was submitted to the U.S. Food and Drug Administration (FDA) in March 2024, which was accepted in June 2024. The rolling submission of a Biologics License Application (BLA) for maintenance dosing of a subcutaneous injection formulation, which is being developed to enhance convenience for patients, was initiated in the U.S. under Fast Track status in May 2024.
Since July 2020, the Phase 3 clinical study (AHEAD 3-45) for individuals with preclinical AD, meaning they are clinically normal and have intermediate or elevated levels of amyloid in their brains, is ongoing. AHEAD 3-45 is conducted as a public-private partnership between the Alzheimer's Clinical Trial Consortium that provides the infrastructure for academic clinical trials in AD and related dementias in the U.S, funded by the National Institute on Aging, part of the National Institutes of Health, Eisai, and Biogen. Since January 2022, the Tau NexGen clinical study for Dominantly Inherited AD (DIAD), that is conducted by Dominantly Inherited Alzheimer Network Trials Unit (DIAN-TU), led by Washington University School of Medicine in St. Louis, is ongoing and includes lecanemab as the backbone anti-amyloid therapy.
2. About the Collaboration between Eisai and Biogen for Alzheimer’s Disease
Eisai and Biogen have been collaborating on the joint development and commercialization of AD treatments since 2014. Eisai serves as the lead of lecanemab development and regulatory submissions globally with both Eisai and Biogen co-commercializing and co-promoting the product and Eisai having final decision-making authority.
3. About the Collaboration between Eisai and BioArctic for Alzheimer’s Disease
Since 2005, Eisai and BioArctic have had a long-term collaboration regarding the development and commercialization of AD treatments. Eisai obtained the global rights to study, develop, manufacture and market lecanemab for the treatment of AD pursuant to an agreement with BioArctic in December 2007. The development and commercialization agreement on the antibody lecanemab back-up was signed in May 2015.
4. About Eisai Co., Ltd.
Eisai's Corporate Concept is "to give first thought to patients and people in the daily living domain, and to increase the benefits that health care provides." Under this Concept (also known as human health care (hhc) Concept), we aim to effectively achieve social good in the form of relieving anxiety over health and reducing health disparities. With a global network of R&D facilities, manufacturing sites and marketing subsidiaries, we strive to create and deliver innovative products to target diseases with high unmet medical needs, with a particular focus in our strategic areas of Neurology and Oncology.
In addition, we demonstrate our commitment to the elimination of neglected tropical diseases (NTDs), which is a target (3.3) of the United Nations Sustainable Development Goals (SDGs), by working on various activities together with global partners.
For more information about Eisai, please visit www.eisai.com (for global headquarters: Eisai. Co., Ltd.), us.eisai.com (for U.S. headquarters: Eisai, Inc.) or www.eisai.eu (for Europe, Middle East, Africa, Russia, Australia and New Zealand headquarters: Eisai Europe Ltd.), and connect with us on X (global and U.S), LinkedIn (for global, U.S. and EMEA) and Facebook (global).
5. About Biogen
Founded in 1978, Biogen is a leading biotechnology company that pioneers innovative science to deliver new medicines to transform patients’ lives and to create value for shareholders and our communities. We apply deep understanding of human biology and leverage different modalities to advance first-in-class treatments or therapies that deliver superior outcomes. Our approach is to take bold risks, balanced with return on investment to deliver long-term growth.
The company routinely posts information that may be important to investors on its website at www.biogen.com. Follow Biogen on social media – Facebook, LinkedIn, X, YouTube. The website and social media channels are intended for audiences outside of the UK and Europe.
Biogen Safe Harbor
This news release contains forward-looking statements, about the potential clinical effects of lecanemab; the potential benefits, safety and efficacy of lecanemab; potential regulatory discussions, submissions and approvals and the timing thereof; the treatment of Alzheimer's disease; the anticipated benefits and potential of Biogen's collaboration arrangements with Eisai; the potential of Biogen's commercial business and pipeline programs, including lecanemab; and risks and uncertainties associated with drug development and commercialization. These statements may be identified by words such as "aim," "anticipate," "believe," "could," "estimate," "expect," "forecast," "intend," "may," "plan," "possible," "potential," "will," "would" and other words and terms of similar meaning. Drug development and commercialization involve a high degree of risk, and only a small number of research and development programs result in commercialization of a product. Results in early-stage clinical studies may not be indicative of full results or results from later stage or larger scale clinical studies and do not ensure regulatory approval. You should not place undue reliance on these statements.
These statements involve risks and uncertainties that could cause actual results to differ materially from those reflected in such statements, including without limitation unexpected concerns that may arise from additional data, analysis or results obtained during clinical studies; the occurrence of adverse safety events; risks of unexpected costs or delays; the risk of other unexpected hurdles; regulatory submissions may take longer or be more difficult to complete than expected; regulatory authorities may require additional information or further studies, or may fail or refuse to approve or may delay approval of Biogen's drug candidates, including lecanemab; actual timing and content of submissions to and decisions made by the regulatory authorities regarding lecanemab; uncertainty of success in the development and potential commercialization of lecanemab; failure to protect and enforce Biogen's data, intellectual property and other proprietary rights and uncertainties relating to intellectual property claims and challenges; product liability claims; and third party collaboration risks, results of operations and financial condition. The foregoing sets forth many, but not all, of the factors that could cause actual results to differ from Biogen's expectations in any forward-looking statement. Investors should consider this cautionary statement as well as the risk factors identified in Biogen's most recent annual or quarterly report and in other reports Biogen has filed with the U.S. Securities and Exchange Commission. These statements speak only as of the date of this news release. Biogen does not undertake any obligation to publicly update any forward-looking statements.
References
- Sperling, R., Selkoe, D., Reyderman, L., Youfang, C., Van Dyck, C. (2024, July 28 - August 1). Does the Current Evidence Base Support Lecanemab Continued Dosing for Early Alzheimer’s Disease? [Perspectives Session] Alzheimer's Association International Conference, Philadelphia, PA, United States.
- Cohen S., et al. J Prev Alzheimers Dis.2022;9(3):507-522.
- Morris JC. Neurology. 1993;43(11):2412-4.
- LEQEMBI® (lecanemab-irmb) [package insert]. Nutley, NJ. Eisai Inc.; 2023.
- Amin L, Harris DA. Aβ receptors specifically recognize molecular features displayed by fibril ends and neurotoxic oligomers. Nat Commun. 2021;12:3451. doi:10.1038/s41467-021-23507-z.
- Willis, B., Charil, A., Fox, N., Teunissen, C. (2024, July 28-August 1). Beyond Amyloid Removal with Lecanemab Treatment: Update on Long-Term Fluid Biomarkers. [Featured Research Session] Alzheimer’s Association International Conference, Philadelphia, PA, United States.
- Wildsmith, K., Pallavi, S., Horie, K., Reyderman, K., Charil, A., Kanekivo, M., Yin, H., Li, D., Koyama, A., Dhadda, S. Irizarry, M., Kramer, L. (2024, July 28-August 1). Lecanemab Slows Amyloid-Induced Tau Pathology as Supported by CSF MTBR-tau243 in Clarity AD. [Developing Topic] Alzheimer’s Association International Conference, Philadelphia, PA, United States
- Ono K, Tsuji M. Protofibrils of Amyloid-β are Important Targets of a Disease-Modifying Approach for Alzheimer's Disease. Int J Mol Sci. 2020;21(3):952. doi: 10.3390/ijms21030952. PMID: 32023927; PMCID: PMC7037706.
- Eisai presents full results of lecanemab Phase 3 confirmatory Clarity AD study for early Alzheimer's disease at Clinical Trials on Alzheimer's Disease (CTAD) conference. Available at: https://www.eisai.co.jp/news/2022/news202285.html
- van Dyck. C, et al. Lecanemab in Early Alzheimer's Disease. The New England Journal of Medicine. DOI: 10.1056/NEJMoa2212948. https://www.nejm.org/doi/full/10.1056/NEJMoa2212948.
Photos accompanying this announcement are available at:
https://www.globenewswire.com/NewsRoom/AttachmentNg/dc5e0c69-0f4f-40d2-bd70-9ccfe4fd643e
https://www.globenewswire.com/NewsRoom/AttachmentNg/9f04eced-be00-467f-bb66-1813cfe3fcb2

![]()
